

Extramedullary plasmacytomas are present in 7-18% of multiple myeloma at diagnosis, and up to 13-20% at the time of disease relapse. (Blade J et al., 2011; Varettoni M et al., 2010) A case series in 2010 with 1003 patients found involvement of soft tissues surrounding the axial skeleton in 85% of cases at diagnosis, and 72% of cases at time of relapse. Other sites of involvement included lymph nodes, liver, kidney, airways, skin, breast, and the gastrointestinal tract. (Varettoni M et al., 2010) An extramedullary plasmacytoma leading to Pancoast syndrome has been reported only 3 times in previous literature, in 1979, 1983, and 1984. (Brenner B et al., 1984; Chen KT et al., 1983; Wilson KS et al., 1979) A case of this uncommon presentation is reported here.
The patient is a 70-year-old male with a diagnosis of ISS-3 IgG Kappa multiple myeloma (serum monoclonal protein 10 g/L, Kappa light chain 2356.29 mg/L, free light chain ratio 386.28, bone marrow biopsy 61.8% plasma cells) the year prior to the current presentation. He was not a candidate for autologous stem cell transplant due to poor pulmonary function, and hence had a treatment plan for 9 cycles of cyclophosphamide/bortezomib/dexamethasone (CyBorD), of which 6 were completed. Treatment was then stopped due to a macrocytic hypoproliferative anemia thought to be related to early hypoplasia from prior CyBorD. At this time, he was in complete remission with bone marrow biopsy showing 2.8% plasma cells. His medical history was otherwise significant for coronary artery disease with prior myocardial infarction, previous transient ischemic attack with carotid stenosis and carotid endarterectomy, hypertension, dyslipidemia, spinal stenosis with multilevel degenerative changes most pronounced at L3-4, and osteoarthritis. He had a 30 pack-year smoking history, and continued to smoke cigars.
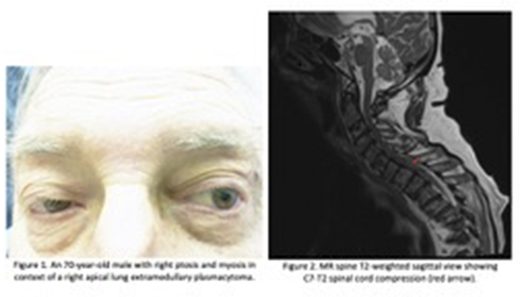
The patient presented to hospital 5 months after completion of the above therapy with 2 weeks of right shoulder pain radiating down the arm, and right hand weakness, numbness, and tingling. He had also noted right lower extremity weakness and numbness with some incontinence. The physical exam was significant for right ptosis and myosis (Figure 1), decreased strength and sensation in the right C8-T1 distribution, inability to lift the right lower extremity off the bed, reduced anal sphincter tone, and a post-void residual volume of 700 mL. CT brain and cervical spine showed new abnormal mass-like tissue within the right hemithorax apical region with apparent extension into the cervicothoracic junction. Given his history of multiple myeloma as well as his smoking history, the mass was thought to either be a primary lung malignancy, or an extramedullary plasmacytoma.
The patient was therefore admitted for ongoing management and diagnostic work-up. He was seen by the inpatient Hematology service, and noted to have progression of his multiple myeloma with Kappa light chain 885.99 mg/L (free light chain ratio 48.67). He was started on pulse steroids with a plan for daratumumab/lenalidomide/dexamethasone (DRd) with dose reduction of the lenalidomide given his prior history of myelosuppression. Further imaging with MR entire spine showed the right lung apical soft tissue mass extending into the epidural space from C7-T2 with severe spinal cord compression and spinal cord edema (Figure 2), as well as epidural extension of disease at L5 resulting in moderate spinal canal stenosis. The patient was then seen by Radiation Oncology and received 8 Gy as a single fraction to the apical lung mass.
Subsequent biopsy of the mass showed a plasma cell neoplasm, Kappa restricted by in-situ hybridization, and compatible with a plasmacytoma. The patient then received two cycles of DRd and thought to be in very good partial response with Kappa light chain 32 mg/L, free light chain ratio 3.8, and resolution of previous apical lung mass and L5 epidural extension on subsequent MR spine.
We document here a rare case of plasmacytoma leading to Pancoast syndrome. Given the difference in therapeutic options and prognosis between an extramedullary plasmacytoma and a primary lung malignancy, it is important to recognize this presentation as a diagnostic possibility, and to pursue relevant investigation and targeted management for the same.
Sharma:Enstasis therapeutics: Current equity holder in private company; Pfizer: Current equity holder in private company; Gilead: Other: shareholder; Contrafect corporation: Current equity holder in private company; Moderna: Other: shareholder.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal